Charcot Foot And Ankle Reconstruction
I was recently asked to give a lecture on Charcot foot and ankle reconstruction and thought that this was an opportune time to write a blog about the new updates and treatments regarding Charcot foot and ankle reconstruction.
Charcot right foot and ankle reconstruction has undergone many types of treatment options over the past 100 years. We have moved far past needing to amputate patients that are affected with Charcot neuroarthropathy, as the first line of treatment. Most of the patients today can do well with reconstruction techniques that allow them to go back into her shoe or to be in a boot.
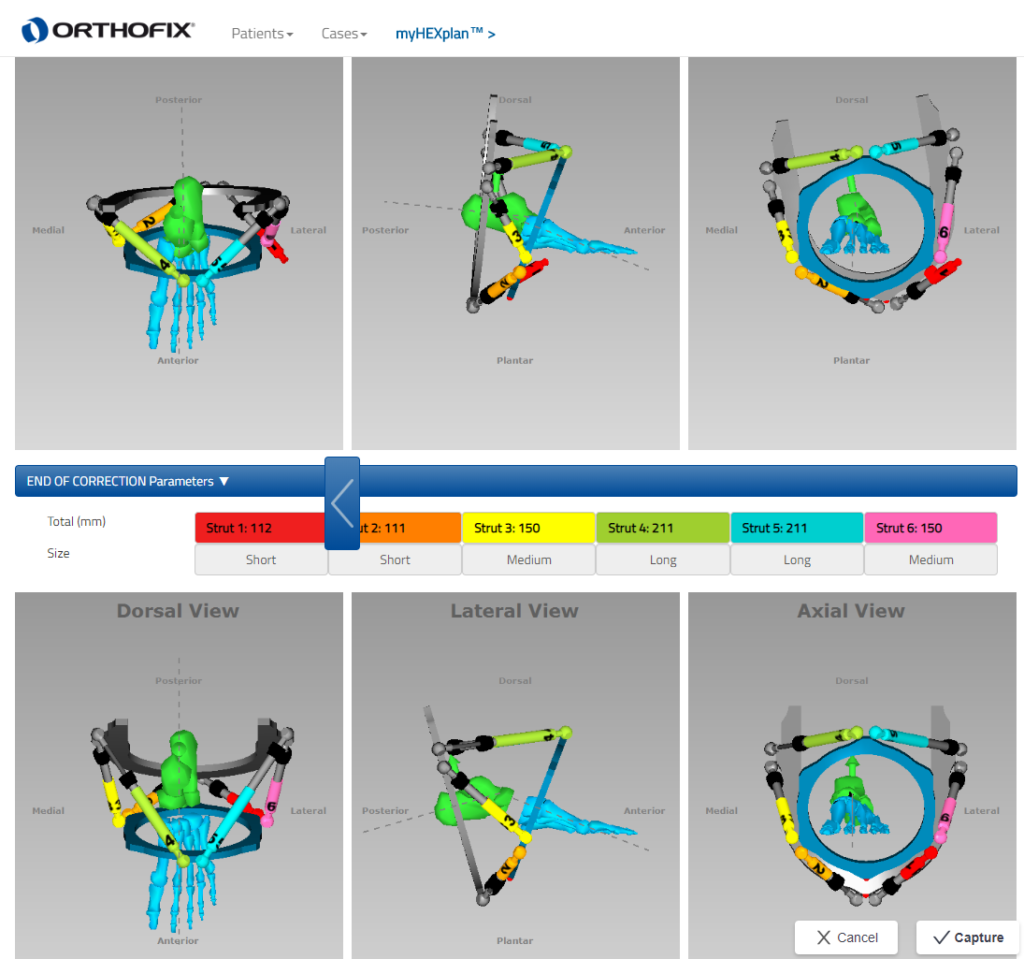
With regard to Charcot foot reconstruction, many advancements have been made in deformity analysis and deformity correction techniques that allow for minimal removal of bone and minimal removal of soft tissue that also allow for maintaining the length of the foot. We used various computer deformity programs that allow us to accurately measure how much bone needs to be removed as well as the precise area of where to make the bone cuts when necessary to reposition the bone after the collapse of a Charcot foot or ankle.
1 of the big advances that we have been able to make with Charcot reconstruction is the beaming technique. Intramedullary beaming of the foot and the ankle allow for a stable structure that makes it easier for the bones to heal. As opposed to in the past when big incisions were made with the application of plates with multiple screws the beams have better strength and from a mechanical standpoint hold a better than plates and screws. Due to the fact that people with Charcot have weakened bones, you will notice that many people Charcot have external fixators applied. Those external fixators are very important in allowing for the beaming procedures to be successful as it prevents 1 from moving the leg around or putting too much weight on their leg while the beams are working. Some people have very large deformities that require a technical gradual deformity correction. Gradual deformity correction is very similar to when 1 has braces for teeth. If one will go to an orthodontist on the orthodontist would say to them, that they were going to take your teeth and crank them into the right spot you get pretty nervous and run out of the office. What you may have expected to hear their input on braces that slowly take the teeth and put them back in the right position. Similar is with the foot and ankle there are many deformities that you cannot put back into the right position and 1 shot and requires a two-stage procedure. That is why you see some of these external fixators with rods next to them that the little rod used to turn very slowly and will slowly correct the foot in the right position. One of the big advancements that we have now with deformity correction are computerized programs that allow us to take exact measurements of where the bones are where the deformity is and we are exactly to make the bone cuts so that the healing is done in the most optimal fashion.
Some of the updates that we find with ankle Charcot are similar to foot Charcot in the sense that the combination of rodding and external fixation is vital for recovery. This comes from the same idea that since the bones are very weakened with Charcot just putting in a plate with some screws is destined for failure. Most cases of ankle Charcot require an intramedullary rodding to hold it in place with an external fixator on top of that. Once the healing is complete and the external fixator can take it off and then you have the rod left and there. Most people with ankle Charcot end up doing better with this technique. Up until the last few years when this technique became more excepted many people had failures of ankle reconstruction secondary to Charcot surgery because this was not to the excepted technique. Now that this is the excepted technique we have gone from a 50% success rate to over 90% success rate.
Lastly, there are many other tricks and techniques that we have found that works very well with making sure the skin heals properly. There have been some great advancements and negative pressure therapy on incisions to help the incisions heal faster. Utilizing all of these techniques we were able to help people with Charcot foot and ankle get back to the regular activities. And at least prevent many amputations that are unnecessary because of these new techniques.
